|
:::
 |
|
|
 |

|
Lumbar Diskectomy |
 |
Lumbar Diskectomy |
|
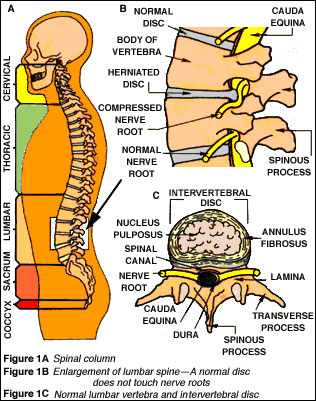
One of the most common types of back surgery is disk removal (diskectomy), the removal of an intervertebral disk, the flexible plate that connects any two adjacent vertebrae in the spine. Intervertebral disks act as shock absorbers, protecting the brain and spinal cord from the impact produced by the body's movements. |
 |
Purpose |
|
|
About 150,000 Americans undergo disk removal each year in the United States. Removing the invertebral disk is performed to treat back pain that has lasted at least six weeks as a result of an abnormal disk and that has not responded to conservative treatment. Surgery is also performed if there is pressure on the lumbosacral nerve roots that causes weakness or bowel or bladder disfunction
As a person ages, the disks between the vertebrae degenerate and dry out, and the fibers holding them in place tear. Eventually, the disk can form a blister-like bulge, compressing nerves in the spine and causing pain. This is called a "prolapsed" (or herniated) disk. If such a disk causes muscle weakness or interferes with bladder or bowel function because it is pressing on a nerve root, immediate surgery to remove the disk may be needed. The aim of the surgery is to try to relieve all pressure on nerve roots by removing the pulpy material from the disk, or the disk itself. If it is necessary to remove material from several nearby vertebrae, the spine may become unsteady. In this case, the surgeon will perform a spinal fusion, removing all the disks between two or more vertebrae and roughening the bones so that the vertebrae heal together. Bone strips taken from the patient's leg or hip may be used to help hold the vertebrae together. Spinal fusion decreases pain but it also decreases spinal mobility.
|
 |
Description |
|
The surgery is done under general anaesthesia, which puts the patient to sleep and affects the whole body. Operating on the patient's back, the neurosurgeon or orthopedic surgeon makes an opening into the vertebral canal, and then moves the dura and the bundle of nerves called the "cauda equina" (horse's tail) aside, which exposes the disk. If a portion of the disk has moved from between the vertebrae out into the nerve canal, it is simply removed. If the disk itself has become fragmented and partially displaced, or not fragmented but bulging extensively, the surgeon will remove the bulging or displaced part of the disk and the part that lies in the space between the vertebrae. |
 |
Preparation |
|
The patient is given an injection an hour before the surgery to dry up internal fluids and encourage drowsiness. |
 |
Aftercare |
|
After the operation, the patient will awaken lying flat and face down, and must remain this way for several days, changing position only to avoid bedsores . There maybe slight pain or stiffness in the back area. Patients should sleep on a firm mattress and avoid bending at the waist, lifting heavy weights, or sitting in one spot for a long time (such as riding in a car).
After surgery, patients can usually leave the hospital on the fourth or fifth day. They must:
- Avoid sitting for more than 15 20 minutes
- Use a reclined chair
- Avoid bending, twisting, or lifting
- Begin gentle walking (indoors or outdoors), gradually increasing
- Begin stationary biking or gentle swimming after two weeks
- Continue exercise for the next four weeks
- Slow down if they experience more than minor pain in the back or leg.
|
 |
Risks |
|
All surgery carries some risk due to heart and lung problems or the anesthesia itself, but this risk is generally extremely small. (The risk of death from general anesthesia for all types of surgery, for example, is only about 1 in 1,600).
The most common risk of the surgery is infection, which occurs in 1 2% of cases. Rarely, the surgery can damage nerves in the lower back or major blood vessels in front of the disk. Occasionally, there may be some residual paralysis of a particular leg or bladder muscle after surgery, but this is the result of the disk problem that necessitated the surgery, not the operation itself.
While disk removals can relieve pain in 90% of cases, there are some people who do not get pain relief, depending on how long they had the condition requiring surgery and other factors. |
 |
Normal results |
|
After about five days, most patients can leave the hospital. They can resume all normal activities, including work, after four to six weeks of recuperation at home.
In properly evaluated patients, there is a very good chance that disk removal will be successful in easing pain. Even in patients over age 60, disk surgery has a "good to excellent" result for 87% of patients. Disk surgery can relieve both back and leg pain, but the greatest pain relief will occur with the leg pain. |
|
|
|
What is It? |
|
Lumbar laminectomy is an operation performed on the lower spine to relieve pressure on one or more nerve roots. The term is derived from lumbar (lower spine), lamina (part of the spinal canal's bony roof), and -ectomy (removal). |
|
Why is it Done? |
|
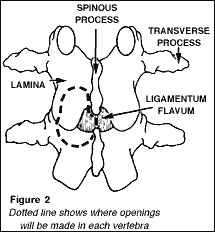
Pressure on a nerve root in the lower spine, often called nerve root compression, causes back and leg pain. In this operation the surgeon reaches the lumbar spine through a small incision in the lower back. After the muscles of the spine are spread, a portion of the lamina is removed (Fig. 2) to expose the compressed nerve root(s).
Pressure is relieved by removal of the source of compression part of the herniated disc, a disc fragment, a tumor, or a rough protrusion of bone, called a bone spur.
|
|
What Happens Afterwards? |
|
Successful recovery from lumbar laminectomy requires that you approach the operation and recovery period with confidence based on a thorough understanding of the process. Your surgeon has the training and expertise to correct physical defects by performing the operation; he and the rest of the health care team will support your recovery. Your body is able to heal the involved muscle, nerve, and bone tissues. Full recovery, however, will also depend on your having a strong, positive attitude, setting small goals for improvement, and working steadily to accomplish each goal. |
|