|
:::
 |
|
|
 |

|
Sciatica |
|
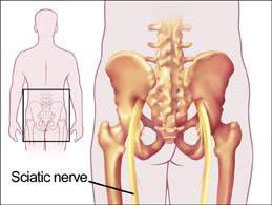 Sciatica, characterized by pain radiating into one or both buttocks and descending the back of the leg, results from compression of the sciatic nerve at the base of the spine or compression of the spinal roots that contribute to the sciatic nerve. This nerve (one for each side of the lower body) is the longest in the peripheral nervous system, extending through the buttocks and down as far as the foot. The pain can occur along its entire length. Sciatica, characterized by pain radiating into one or both buttocks and descending the back of the leg, results from compression of the sciatic nerve at the base of the spine or compression of the spinal roots that contribute to the sciatic nerve. This nerve (one for each side of the lower body) is the longest in the peripheral nervous system, extending through the buttocks and down as far as the foot. The pain can occur along its entire length.
|
|
Causes |
|
Pressure on a sciatic nerve may be due to poor posture, muscle strain, pregnancy, being overweight, wearing high heels or sleeping on a too-soft mattress. It can also result from a slipped disc or inflammation of the sciatic nerve, in some cases caused by osteoarthritis. |
|
Lumbar spine disorders known to cause sciatic nerve compression include the following |
|
|
- Herniated discs are the most common cause of sciatica in the lumbar spine.
- Degenerative Disc Disease, a natural biological process associated with aging, is known to cause disc weakness that can be a precursor to a disc herniation.
- Lumbar Spinal Stenosis is a narrowing of one or more neural passageways due to disc degeneration and/or facet arthritis. The sciatic nerve may become impinged as a result of these changes.
- Isthmic Spondylolisthesis results from a stress fracture often at the 5th lumbar vertebra (L5). The fracture combined with disc space collapse may allow the vertebra to slip forward on the first sacral segment (S1). The slippage may cause the L5 nerve root to become pinched as it leaves the spine.
- Spinal Tumors and Infections are other disorders that may compress the sciatic nerve, but this is rare.
- There are other conditions, which may occur, and may mimic true sciatica but these are difficult to diagnose.
|
|
Symptoms |
- Pain radiating through your buttock, down the back of your thigh and leg, often to your foot. The pain can be sharp or dull, shooting or burning, intermittent or continuous. It usually affects just one side of the body. Coughing, sneezing, bending or lifting may make it worse.
- In some cases, numbness and weakness of the affected area.
|
| |
Extending from the tailbone to the toes, the two branches of the sciatic nerve register sensation including pain every time the leg is stimulated. Continuous pressure on the nerve, perhaps from a slipped vertebral disc or a fetus in the womb, can send a stream of pain messages along the length of the nerve; the intensity of the pain can range from mild to debilitating |
|
Diagnostic and Test Procedures |
| |
The physician's examination includes the patient's medical history, a review of current medications, a physical and neurologic examination and, if warranted, x-rays, CT scan and/or MRI. A proper diagnosis requires an analysis of the patient's pain. The patient is often provided a Pain Diagram to illustrate pain distribution and sensation (eg, tingling and burning). |
|
Prevention |
- Sleep on a firm mattress on your back or side with your knees bent; avoid sleeping on your stomach.
- Adjust the height of your chair so your feet are flat on the floor and your knees are a little higher than your hips; make a habit of sitting with both feet flat on the floor instead of crossing your legs.
- Make sure your chair has firm back support, and sit with your butt against the back of the chair, with your weight resting on the bones of your buttocks. Don't slouch or slump in the chair.
|
|
Treatment |
|
|
|
Non-Surgical Treatment
- Sciatica often responds well to non-operative forms of treatment and rarely requires surgical intervention. Time, non-steroidal anti-inflammatory (NSAIDs) medication, short-term use of a narcotic for acute pain, lumbar injections, and physical therapy are beneficial.
- Although short-term bed rest is recommended during the acute phase, some activity is good. In this scenario "activity" is defined as being up for periods of time that will not cause severe pain. Prescribed exercise may include light stretching, walking, and aerobic type exercise.
Surgery
Surgery is not for all patients. However, in some situations, surgery may be indicated. Patients who have followed a non-surgical course of treatment for four to six weeks without relief certainly require a re-evaluation by their physician. If a MRI scan reveals a herniated disc or spinal stenosis, surgery may provide relief of the leg pain. The type of surgical procedure is dependent in part on the patient's condition and diagnosis |
|
Recovery |
|
Whether treatment for sciatica is non-operative or surgical, it is always wise to follow the instructions provided by the doctor and/or physical therapist.
Work toward relieving unnecessary mechanical stress to the spine. For example, when standing, alternate resting one foot on a stool. When driving, place a small pillow or rolled towel behind the back to maintain natural spinal curvature. At bedtime, sleep on the back with a pillow under the knees or between the knees if sleeping on the side. Strive to eat healthy, work toward your ideal body weight, and avoid smoking. These lifestyle changes all benefit the spine's health. |
|
|
|